Radiofrequency Ablation (RFA) vs. Microwave Ablation (MWA)
for Thyroid Treatment
The latest Microwave vs Radiofrequency Ablation (RFA) research suggests that RFA may be more effective at longer follow-up periods. We’ve gathered the insights you need to better understand the difference between these two treatment modalities. Learn more about the differences between RFA and Microwave Ablation for thyroid nodules below.
Microwave Ablation is not the same as Radiofrequency Ablation, though they share similarities. Both procedures aim to destroy targeted tissue, which the body eliminates as waste. However, microwave ablation delivers energy at a higher frequency than RFA via direct oscillation of electromagnetic energy. In contrast, RFA uses an oscillating current on the radiofrequency spectrum.
As a result, microwave thyroid ablation offers higher power and a larger ablation zone compared to RFA. While advantageous for treating larger organs like the liver, MWA’s intensity can pose challenges for structures like the thyroid.
More precise marginal venous ablation is crucial for effective volume reduction. Likewise, precision is essential for preventing marginal regrowth. A higher level of accuracy can be found using the radiofrequency ablation procedure, ideal for smaller, more delicate structures such as the thyroid.
RFA is often considered a safer and more precise option compared to microwave thyroid ablation. The lower power of ablation reduces the risk of complications. As a result, practitioners newer to minimally invasive thyroid treatment learn faster and achieve consistently positive outcomes.
Microwave Ablation and RFA in the Literature: Key Insights
The most recent research from Baek et al. and Zufry et al. revealed the following insights about RFA and microwave ablation for the thyroid:
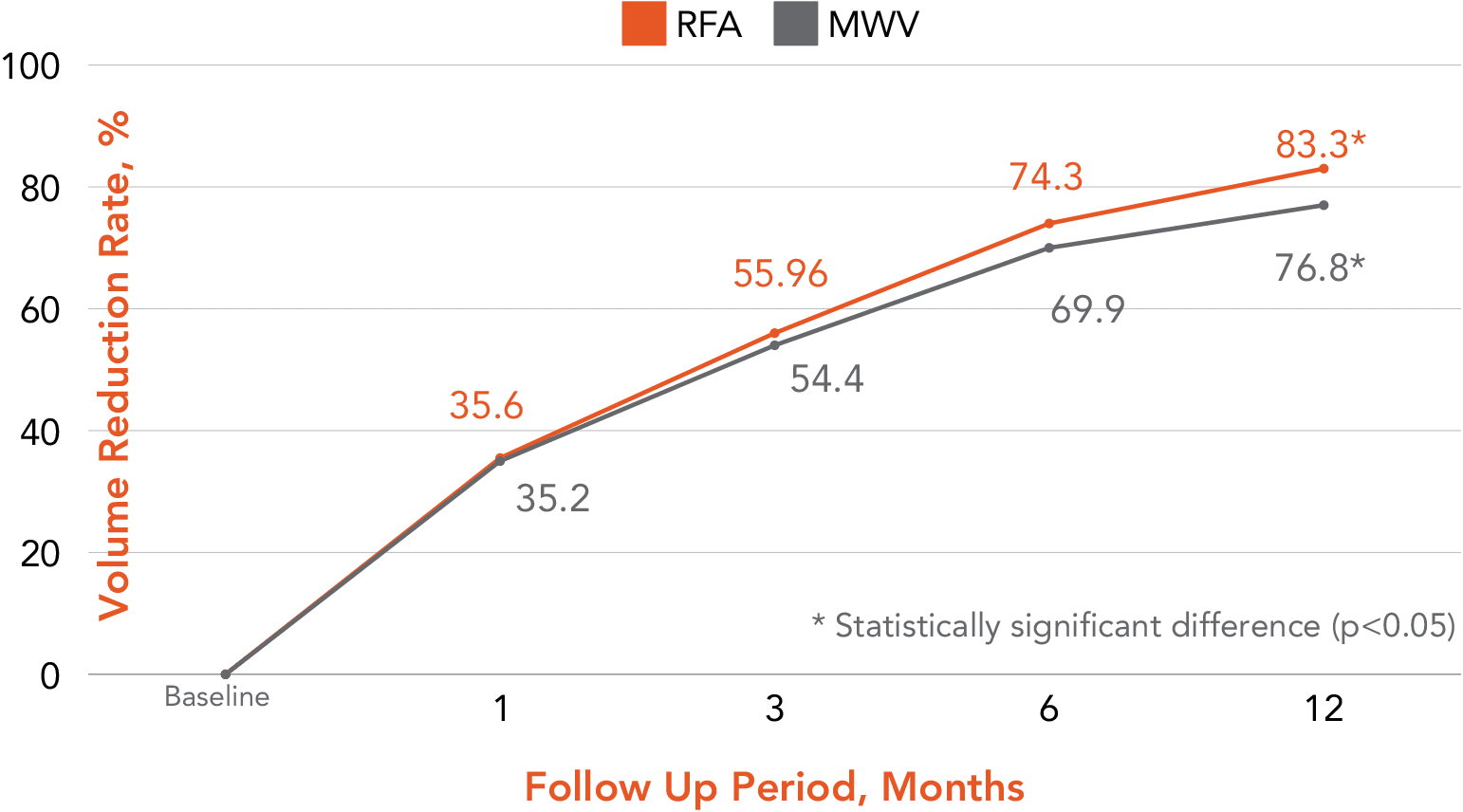
Fig. 2 The trends in pooled volume reduction rates for thyroid nodules treated with RFA and MWA. There was a significant difference in the pooled VRR at 12 months between RFA and MWA (83.34% vs 76.89%, respectively, p = .02). MWA, microwave ablation; RFA, radiofrequency ablation; VRR, volume reduction rate.
RFA showed a significantly higher VRR of 83.3% compared to MWA of 76.8% at 12 months despite there being no significant difference in the pooled baseline nodule volume between the groups.
The VRR of ablated nodules is likely to be higher in the RFA group because tissue carbonized during MWA does not dissolve well.
In MWA, a higher likelihood of remaining viable tissue, particularly at the margins of the ablated area, leads to a lower initial ablation ratio. In turn, that results in a reduced final VRR.
It’s crucial to note that the benefits of Radiofrequency Ablation are more pronounced for practitioners with less experience. Thus, RFA is the preferred procedure for clinicians new to thyroid ablation.
RFA demonstrated a significantly higher VRR than MWA in clinicians with less than 10 years of experience
Voice changes are less frequent with RFA than with MWA, probably due to higher ablation power with microwave ablation.
MWA often leads to carbonization in ablated lesions due to temperatures over 150 °C, which is less common in RFA where temperatures do not exceed 110 °C
This is the perfect time to pursue clinical training and implement this efficacious modality into your practice.
Research suggests that thyroid RFA patients consistently experience more favorable long-term outcomes compared to MWA patients. Lower energy delivery and more predictable ablation margins make it safer to treat delicate thyroid nodules.
Electrodes used in the RFA procedure are smaller, thinner, and more agile than microwave antennas. As a result, they do not require an incision, leading to more comfortable care and efficient treatment.
Ultimately, RFA patients have lower symptom and cosmetic scores when compared to MWA patients. They have faster treatment times and require less follow-up care compared to patients treated via MWA or surgery.
Are you interested in offering your patients the most effective long-term solution for the reduction of benign thyroid nodules? Connect with us to discuss your next steps in implementing RFA in your clinical practice.
Lim, H., Cho, S. J., & Baek, J. H. (2025). Comparative efficacy and safety of radiofrequency ablation and microwave ablation in benign thyroid nodule treatment: a systematic review and meta-analysis. European radiology, 35(2), 612–623. https://doi.org/10.1007/s00330-024-10881-7
Zufry, H., & Hariyanto, T. I. (2024). Comparative Efficacy and Safety of Radiofrequency Ablation and Microwave Ablation in the Treatment of Benign Thyroid Nodules: A Systematic Review and Meta-Analysis. Korean journal of radiology, 25(3), 301–313. https://doi.org/10.3348/kjr.2023.1004
See how safe and effective STARMED’s industry-leading equipment is in practice.
By submitting this form, you consent to receive marketing emails from STARMED America at the email provided. You can unsubscribe at any time. Please see our privacy policy for more information.